A sine wave electrocardiogram (ECG) signifies a critical medical emergency, often indicating severely elevated potassium levels (hyperkalemia). This informational guide provides healthcare professionals with a concise, step-by-step approach to recognizing, treating, and managing this life-threatening condition.
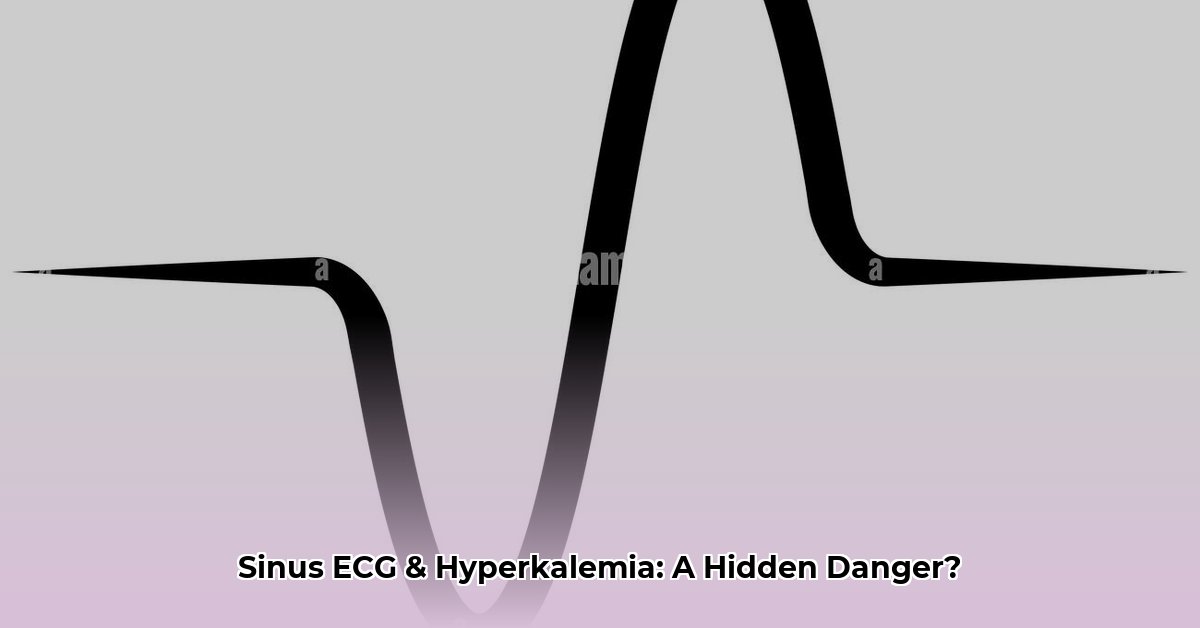
Key Features: Absence of P-waves, widened and merged QRS and T-waves, resulting in a sinusoidal waveform.(Please replace “sine-wave-ecg.jpg” with an actual high-quality, labeled image.)
A sine wave ECG appears as a smooth, undulating waveform, replacing the distinct P, QRS, and T waves of a normal ECG. This pattern suggests a profound disturbance in cardiac electrical activity, primarily caused by hyperkalemia. Prompt recognition and intervention are crucial to prevent imminent cardiac arrest.
Causes of Sine Wave ECG (Hyperkalemia)
Hyperkalemia disrupts the delicate balance of electrolytes essential for normal heart rhythm. The pathophysiology involves potassium’s influence on cardiac cell membrane potential, causing:
Peaked T-waves: An early sign of mild to moderate hyperkalemia.
Sine Wave Pattern: The ultimate consequence of severe hyperkalemia, representing the merging of the QRS complex and T-wave, signifying severely impaired ventricular function.
Several factors contribute to hyperkalemia, including:
Renal Failure: Impaired potassium excretion by the kidneys.
Medications: Certain drugs, such as ACE inhibitors and potassium-sparing diuretics, can elevate potassium levels.
Tissue Breakdown: Trauma, burns, or rhabdomyolysis release intracellular potassium.
A sine wave ECG represents a pre-terminal cardiac rhythm, indicating a high risk of imminent cardiac arrest. The prognosis depends on the speed and effectiveness of treatment. Delayed intervention significantly increases the risk of mortality.
Emergency Treatment: A Step-by-Step Guide
Every second counts when encountering a sine wave ECG. Here’s a structured approach:
Ensure ABCs and IV Access: Stabilize airway, breathing, and circulation while establishing intravenous access.
Cardioprotection (Calcium): Administer calcium gluconate 1-2 g IV over 2-5 minutes. This stabilizes the cardiac membrane, reducing the risk of arrhythmias. Repeat as needed.
Potassium Redistribution:
Insulin/Glucose: Administer 10 units of regular insulin IV push along with 25-50g of dextrose (e.g., 50 ml of 50% dextrose solution) IV push. This shifts potassium intracellularly. Monitor blood glucose closely.
Albuterol: Nebulize 10-20 mg over 10 minutes. This may also help shift potassium intracellularly, especially for patients unable to tolerate glucose. The effectiveness of albuterol in this context is under continued investigation.
Potassium Removal:
Loop Diuretics (Furosemide): Administer 40-80 mg IV push. This promotes renal potassium excretion. Effectiveness is limited in renal failure.
Sodium Polystyrene Sulfonate (Kayexalate): Administer orally or rectally. Binds potassium in the gut for excretion. This therapy acts slowly and might not be suitable for acute emergencies.
Hemodialysis: The most effective method for rapid potassium removal, essential in severe cases and renal failure.
Treatment
Dose/Route
Action
Monitoring
Calcium Gluconate
1-2g IV over 2-5 min
Stabilizes cardiac membrane
ECG, Calcium levels
Insulin
10 units IV push
Shifts potassium intracellularly
Blood Glucose
Dextrose (50%)
25-50g IV push
Prevents hypoglycemia with insulin
Blood Glucose
Albuterol
10-20mg Nebulized
May shift potassium intracellularly
Heart rate, Potassium levels
Furosemide
40-80 mg IV push
Increases renal potassium excretion
Potassium levels, Urine output
Kayexalate
Oral/Rectal
Binds potassium in gut
Potassium levels
Hemodialysis
As needed
Removes potassium directly from the blood
Potassium levels, Fluid balance
Differential Diagnosis
While hyperkalemia is the primary cause, other rare conditions may mimic a sine wave ECG:
Severe Hypothermia: Profoundly low body temperature can alter cardiac conduction, sometimes producing a similar pattern.
Tricyclic Antidepressant Overdose: These drugs can disrupt cardiac conduction, potentially leading to a sine wave-like appearance.
It is crucial to assess the clinical context and consider alternative diagnoses if potassium levels are normal.
Long-Term Management and Prevention
Preventing hyperkalemia recurrence involves:
Identify and Manage Underlying Cause: Address contributing factors like renal failure, medications, or metabolic disorders.
Dietary Potassium Restriction: Limit intake of high-potassium foods, especially in patients with chronic kidney disease. A registered dietitian can provide individualized guidance.
Medication Review: Adjust or discontinue medications that may contribute to hyperkalemia.
Regular Monitoring: Monitor potassium levels and ECGs, especially in high-risk individuals.
Conclusion
A sine wave ECG is a dire warning of severe hyperkalemia and impending cardiac arrest. Rapid recognition and immediate treatment following the outlined steps are crucial for patient survival. Long-term management focuses on identifying and addressing underlying causes, dietary modifications, and medication review to prevent recurrence.
Disclaimer: This information is for educational purposes only and should not be considered medical advice. Always consult with a qualified healthcare professional for diagnosis and treatment.
I am a writer who loves renewable energy, with a focus on sustainable living, renewable energy, and eco-friendly innovation. With a passion for environmental awareness and a desire to explore the latest trends in green technology, corporate sustainability, and climate action. Through in-depth storytelling