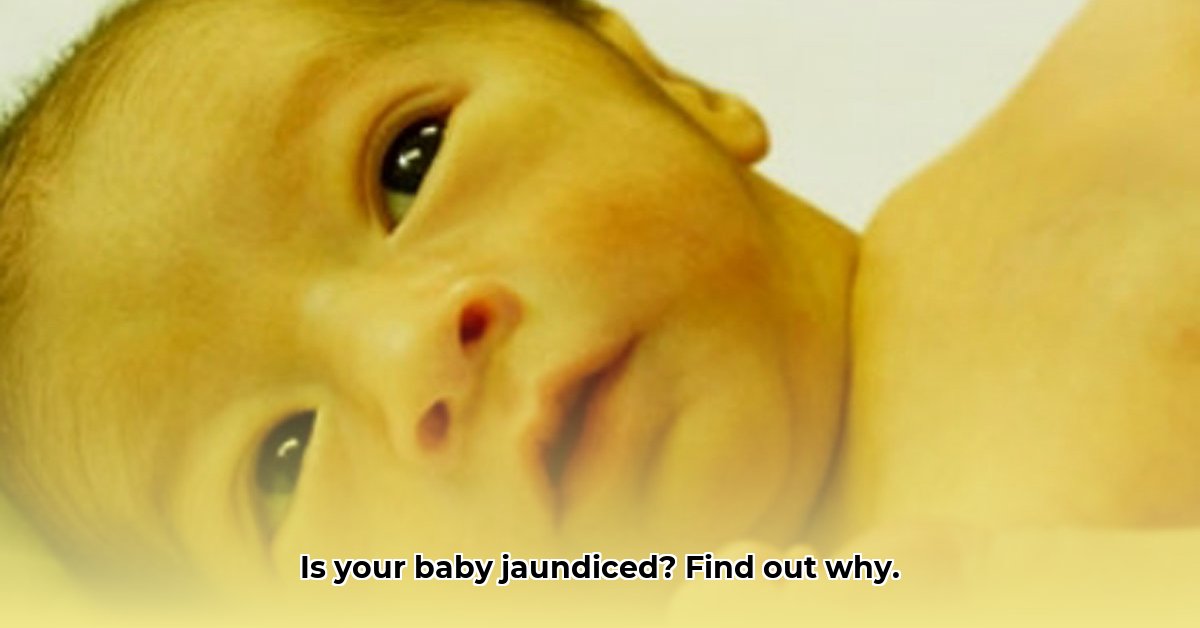
Bringing a new baby home is a joyous occasion, but sometimes, unexpected health concerns like jaundice can arise. Jaundice, characterized by a yellowish tint to your baby’s skin and eyes, is common in newborns. Understanding what jaundice means, its causes, how it’s tested, and treatment options can empower you to feel more confident and less stressed during this time. This guide provides essential information to help you navigate your baby’s jaundice and understand when to seek medical attention, ensuring the best possible care for your little one. For more on non-invasive testing, see information on non-invasive bilirubin tests.
Understanding Your Baby’s Jaundice Results: Bilirubin Levels and What They Mean
Jaundice is a frequent topic for new parents, especially during the first few weeks of a baby’s life. While the term can be concerning, jaundice is often harmless and temporary. This section clarifies the condition, helping you grasp what the jaundice test results signify for your baby’s health and guiding your understanding of appropriate next steps. Understanding bilirubin, the core indicator, helps you navigate the complexities with greater knowledge.
What is Jaundice and Why Does it Happen? Examining Liver Function
Jaundice is characterized by a yellowish tint visible on the baby’s skin and the whites of their eyes. This yellowing is due to a buildup of bilirubin, a yellow substance produced during the normal breakdown of old red blood cells. The body acts like a recycling center, breaking down and replacing blood cells, with bilirubin as a byproduct. The liver typically processes and eliminates bilirubin efficiently. However, in newborns, the liver might not be fully developed, which can lead to a temporary backlog of bilirubin, resulting in jaundice. This immaturity is a temporary phase, and understanding its impact is critical for parents.
Bilirubin: Understanding the Yellow Culprit and Its Role in Newborn Health
Bilirubin results from the breakdown of hemoglobin, the protein in red blood cells responsible for carrying oxygen throughout the body. This process generates bilirubin, and a newborn’s liver may not process it as efficiently as adult livers. This inefficiency can lead to a temporary increase in bilirubin levels. Therefore, the intensity of jaundice often reflects the amount of bilirubin present in your baby’s system, making bilirubin levels a primary indicator of jaundice severity.
Two Sides of Jaundice: Physiological vs. Pathological and Associated Risk Factors
There are two primary types of jaundice: physiological and pathological. Physiological jaundice is the more common type and isn’t usually a cause for major concern. This temporary condition typically resolves as the baby’s liver matures, becoming more efficient at processing bilirubin, generally within the first two weeks of life.
On the other hand, pathological jaundice indicates an underlying health issue such as a liver problem, a blood incompatibility between mother and child, a red blood cell issue, or an infection. This type may appear earlier, be more severe, and may require medical intervention. Causes of pathological jaundice include:
Blood Type Incompatibility (Rh or ABO): When the mother and baby have different blood types, the mother’s antibodies can attack the baby’s red blood cells, causing a rapid breakdown and increased bilirubin.
Genetic Conditions: Conditions like Glucose-6-Phosphate Dehydrogenase (G6PD) deficiency can cause red blood cells to break down faster.
Infections: Infections can impair the liver’s ability to process bilirubin.
Biliary Atresia: A rare condition where the bile ducts are blocked, preventing bilirubin from being excreted.
Cephalohematoma: A collection of blood under the scalp, often from a difficult birth, which can lead to increased bilirubin as the blood is reabsorbed.
Differentiating between the two types is crucial, making understanding your baby’s test results vital.
Spotting the Signs: Recognizing Jaundice and Its Variations Based on Skin Tone
Jaundice typically starts on the face before spreading across the body, but recognizing it can be challenging. The visibility of jaundice fluctuates based on a baby’s skin tone. Babies with darker skin might display yellowing more prominently in the whites of their eyes, and the palms of their hands and soles of their feet. To check for jaundice, gently press on your baby’s forehead or nose. If the skin looks yellow after you release the pressure, your baby may have jaundice. Always contact your pediatrician if you notice any yellowing for an accurate assessment, particularly given variations in appearance based on skin tone and individual health factors.
Testing and Diagnosis: Decoding the Numbers and Interpreting Results
Your pediatrician will likely order a blood test to measure your baby’s bilirubin levels, measuring both total and direct bilirubin. A higher level of total bilirubin indicates more bilirubin is present, while direct bilirubin measures the amount already processed by the liver. Direct bilirubin levels are typically low.
Doctors might also use transcutaneous bilirubinometry (TcB), a non-invasive test using a special device to measure bilirubin levels in your baby’s skin. This test provides a quick estimate without needing a blood draw, but blood tests are more accurate. Your doctor will interpret the results considering your baby’s age (in hours), weight, gestational age, feeding method, and overall health to determine the severity and the appropriate treatment.
General Guidelines for Bilirubin Levels:
Bilirubin Level (mg/dL)
Severity
Possible Next Steps
Mild (Below threshold)
Physiological Jaundice
Close monitoring, frequent feedings
Moderate (Threshold to moderate)
Requires Monitoring
May need phototherapy, close monitoring
Severe (above moderate)
Pathological Jaundice
May need phototherapy or exchange transfusion
Note: These ranges are approximate and depend on your baby’s age and other factors. Your doctor will use age-specific charts developed by the American Academy of Pediatrics for accurate interpretation. These charts plot bilirubin levels against the baby’s age in hours and consider risk factors.
Treatment Options: Gentle Approaches Like Phototherapy and Exchange Transfusion Explained
If your baby’s bilirubin levels are elevated, your doctor will likely recommend phototherapy, placing your baby under special blue lights to break down the bilirubin into a water-soluble form that the body can eliminate through urine and stool. Phototherapy is generally safe and effective. During phototherapy, the baby’s eyes are protected with special eye shields.
In rare cases involving very high bilirubin levels that don’t respond to phototherapy, an exchange transfusion might be necessary. This procedure removes some of the baby’s blood and replaces it with donor blood containing lower bilirubin levels. This measure is usually reserved for dangerously high levels posing a significant health risk to the baby, specifically to prevent kernicterus, a rare type of brain damage that can result from untreated jaundice.
Home Care: Supporting Your Little One with Frequent Feedings and Monitoring
While medical interventions can be critical, much of the care for a baby with jaundice can be administered at home through simple yet important actions:
Frequent feedings: Frequent feeding, either breastfeeding or formula feeding (every 2-3 hours), is essential, as it helps remove bilirubin through bowel movements, aiding the body’s natural processes. Aim for 8-12 feedings per day.
Monitoring: Keep a close watch on your baby’s skin color and note any changes in the yellowing that may signal a need for further intervention. Check the color in natural light. Also, monitor your baby’s temperature, activity level, and feeding habits.
Sunlight Exposure (with caution): Brief exposure to indirect sunlight can help break down bilirubin. However, avoid direct sunlight, which can cause sunburn. A few minutes of exposure near a window is sufficient, but this should not replace prescribed phototherapy. Always consult your pediatrician before using sunlight as a treatment.
Follow-up: Attend all scheduled appointments with your pediatrician to closely monitor your baby’s progress and make any necessary adjustments to the treatment plan. Follow-up appointments are usually scheduled within 24-48 hours after discharge from the hospital.
When to Call for Help: Recognizing Urgent Situations and Warning Signs
While physiological jaundice is generally mild, it’s essential to be aware of signs indicating your baby needs immediate medical attention:
Increasing jaundice: When the yellowing is becoming progressively more intense, especially if it spreads to the abdomen or legs.
Lethargy or poor feeding: If your baby seems unusually sleepy, lethargic, and feeds poorly, refuses to feed, or is not gaining weight, it is essential to get immediate help.
High-pitched cry: An unusually shrill or persistent cry can be a warning sign.
Fever: Any sign of fever (temperature above 100.4°F or 38°C) warrants immediate attention.
Difficult to wake or is very sleepy: If your baby is difficult to wake up or is excessively sleepy.
Arched back: If your baby arches their back or neck, it could be a sign of kernicterus.
Dark urine or pale stools: These can indicate a problem with bilirubin processing.
These warning signs should prompt immediate action to avert potential complications.
Open Communication: Your Partner in Care with Pediatricians
Remember that every baby is unique. Your pediatrician is your best resource for understanding your baby’s specific test results and determining the most appropriate treatment course. Don’t hesitate to
I am a writer who loves renewable energy, with a focus on sustainable living, renewable energy, and eco-friendly innovation. With a passion for environmental awareness and a desire to explore the latest trends in green technology, corporate sustainability, and climate action. Through in-depth storytelling